
March 2025 Medical Image of the Month: An Unusual Case of Pulmonary Infarction
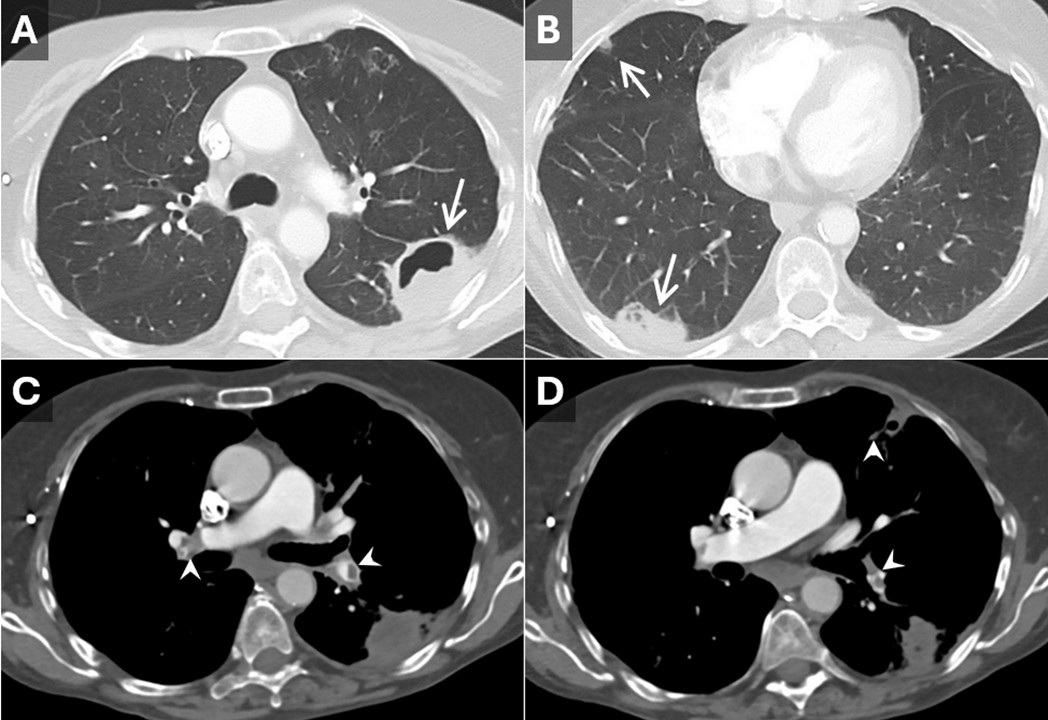
 Figure 1. Axial reconstructions from a contrast-enhanced CT angiogram of the chest performed according to pulmonary embolism protocol. Lung window reconstructions (A,B) demonstrate multiple peripheral lesions with variable degrees of cavitation (arrows). Vascular window reconstructions (C,D) demonstrate pulmonary artery filling defects consistent with pulmonary emboli (arrowheads) which are associated with the cavitary lesions. To view Figure 1 in a separate, enlarged window click here.
Figure 1. Axial reconstructions from a contrast-enhanced CT angiogram of the chest performed according to pulmonary embolism protocol. Lung window reconstructions (A,B) demonstrate multiple peripheral lesions with variable degrees of cavitation (arrows). Vascular window reconstructions (C,D) demonstrate pulmonary artery filling defects consistent with pulmonary emboli (arrowheads) which are associated with the cavitary lesions. To view Figure 1 in a separate, enlarged window click here.
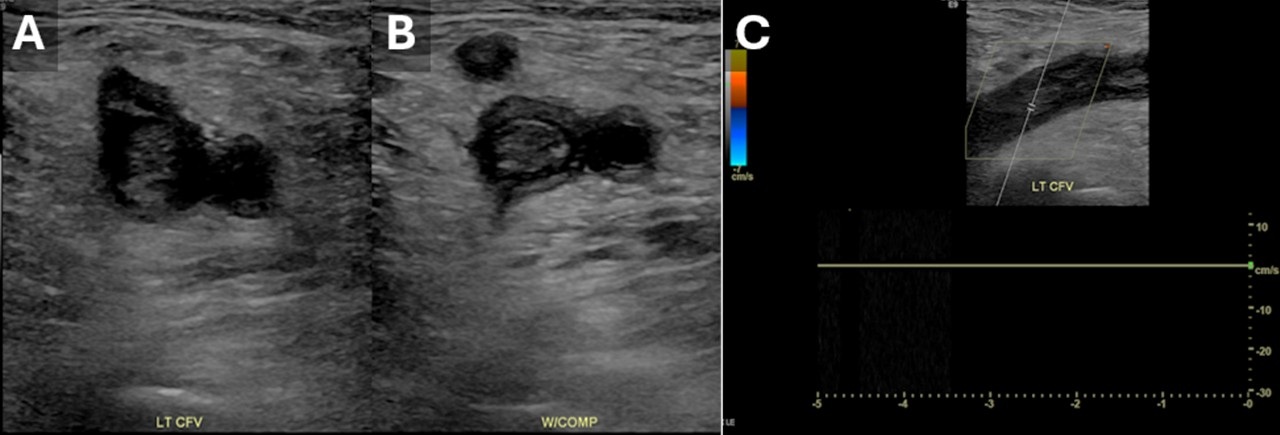
 Figure 2. Lower extremity duplex venous ultrasound performed to evaluate for deep venous thrombosis (DVT). Short axis 2D images through the left common femoral vein (CFV) without (A) and with (B) compression are positive for DVT. Color doppler imaging through the left CFV (C) fails to demonstrate any blood flow. Findings are consistent with left CFV DVT, the likely cause of the patient’s pulmonary emboli. To view Figure 2 in a separate, enlarged window click here.
Figure 2. Lower extremity duplex venous ultrasound performed to evaluate for deep venous thrombosis (DVT). Short axis 2D images through the left common femoral vein (CFV) without (A) and with (B) compression are positive for DVT. Color doppler imaging through the left CFV (C) fails to demonstrate any blood flow. Findings are consistent with left CFV DVT, the likely cause of the patient’s pulmonary emboli. To view Figure 2 in a separate, enlarged window click here.
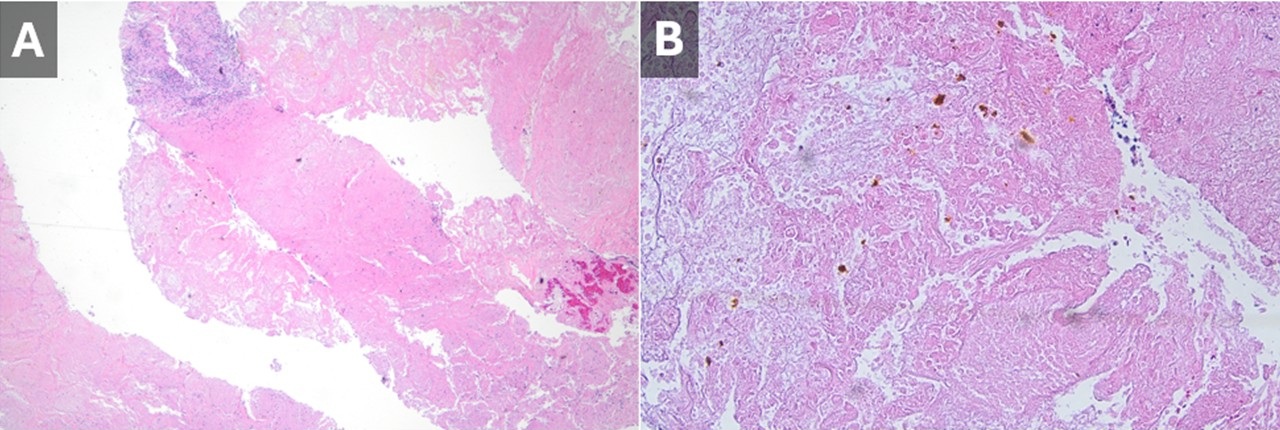
 Figure 3. Due to the high level of concern for septic emboli, one of the lesions was biopsied. Low-power (A) and high-power (B) Hematoxylin and Eosin (H&E) stains of a core biopsy specimen demonstrate findings consistent with a bland pulmonary infarct including hemorrhages, necrosis, and fibrin deposition. To view Figure 3 in a separate, enlarged window click here.
Figure 3. Due to the high level of concern for septic emboli, one of the lesions was biopsied. Low-power (A) and high-power (B) Hematoxylin and Eosin (H&E) stains of a core biopsy specimen demonstrate findings consistent with a bland pulmonary infarct including hemorrhages, necrosis, and fibrin deposition. To view Figure 3 in a separate, enlarged window click here.
A 62-year-old woman with a history of hypertension, hypothyroidism, alcohol use, unexplained weight loss, and anorexia (for which she had been prescribed megestrol 3 months earlier) presented with alarming swelling in her left lower extremity. The swelling started in the left leg but progressively involved the entire left lower extremity over the course of a week. Patient also reported worsening chest pain and shortness of breathing starting 3 days prior to presentation. No cough or hemoptysis, no fevers or chills. She had a 45 pack-year smoking history. Her physical exam showed sinus tachycardia with heart rate 108 beats per minute, blood pressure 110/70 mm Hg, SpO2 was reading at 88% on room air. There was no jugular venous distention. Her heart sounds were normal, and her chest was clear upon auscultation. Patient was placed on supplemental oxygen. A chest X-ray (CXR) revealed mass-like cavitary lesions in both lungs. Routine laboratory work was pertinent for elevated D-dimer. A subsequent CT angiogram of the chest (Figure 1 A-D) demonstrated bilateral pulmonary emboli as well as multiple cavitary mass-like lesions in lungs which have an appearance concerning for septic emboli. A CT of the abdomen and pelvis was unremarkable.
The patient was admitted to the step-down unit, and blood cultures and sputum cultures were collected. Empiric antibiotic therapy was initiated. Venous Doppler confirmed extensive deep vein thrombosis (DVT) in the left lower extremity (Figure 2 A-C), and anticoagulation with a heparin drip was started. Connective tissue disease and vasculitis panels yielded negative results. A 2D echocardiogram showed a normal ejection fraction with no evidence of right ventricular strain or vegetations. Due to the lesions' location and concerns regarding atypical infection versus malignancy, a percutaneous CT-guided biopsy was performed after temporarily halting anticoagulation. Pathology confirmed pulmonary infarction changes, including hemorrhages, necrosis, and fibrin deposition (Figure 3 A-B) without any signs of infection. Her blood cultures remained negative and sputum cultures grew normal flora. Antibiotic therapy was discontinued. The patient had reported a recent workup for unintentional weight loss by her primary care physician, including a colonoscopy prior to her hospital admission, which was unremarkable. Additionally, a mammogram was negative for suspicious lesions.
Cavitary lung infarctions, though rare, present significant diagnostic and management challenges and should be considered in the differential diagnosis of cavitary lung disease, especially in the setting of thromboembolism. In this case, the patient’s unexplained weight loss and anorexia initially raised concern for potential malignancy. However, her CT abdomen, recent mammogram, and colonoscopy were all within normal, making neoplastic causes less likely. Although her history of alcoholism could predispose her to immunosuppression, aspiration pneumonias, and atypical infections (which can also present with cavitary lung lesions), the patient did not exhibit symptoms or signs of infection. Her blood and sputum cultures remained negative throughout the hospital admission. On the other hand, the initiation of Megestrol therapy likely triggered left lower extremity deep vein thrombosis (DVT), which led to subacute thromboembolic events and pulmonary infarctions. This was consistent with the pathologic findings.
Cavitary lung lesions can result from a variety of pathologies, making the diagnosis of the underlying etiology challenging. Cavitary lung infarctions, though rare, are a known complication of pulmonary embolism (PE). Studies by Knox et al. (1), He et al. (2 ), Scharf et al. (3), and Wilson et al. (4) highlight the complexity of diagnosing and managing cavitary lung infarctions, emphasizing the need for individualized diagnostic approaches, particularly when clinical presentations are ambiguous. This case emphasizes the importance of recognizing this association in relevant clinical scenarios while systematically excluding other potential causes. An individualized diagnostic approach, including integrating clinical findings with advanced imaging, laboratory evaluation, and, when necessary, biopsy, is vital for accurate diagnosis and tailored management
Abdulmonam Ali, MD
Pulmonary & Critical Care
SSM Health
Mount Vernon, IL USA
References
- Knox KS, Arteaga VA. Medical image of the week: PE with infarct and pulmonary cavitation. Southwest J Pulm Crit Care. 2014;9(6):333-4. [CrossRef]
- He H, Stein MW, Zalta B, Haramati LB. Pulmonary infarction: spectrum of findings on multidetector helical CT. J Thorac Imaging. 2006 Mar;21(1):1-7. [CrossRef] [PubMed]
- Scharf J, Nahir AM, Munk J, Lichtig C. Aseptic cavitation in pulmonary infarction. Chest. 1971 Apr;59(4):456-8. [Crossref][PubMed]
- Scharf J, Nahir AM, Munk J, Lichtig C. Aseptic cavitation in pulmonary infarction. Chest. 1971 Apr;59(4):456-8. [CrossRef] [PubMed]
 Post a Comment
Post a Comment

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}