
February 2025 Medical Image of the Month: Unexpected Complications of Transjugular Intrahepatic Portosystemic Shunt (TIPS)

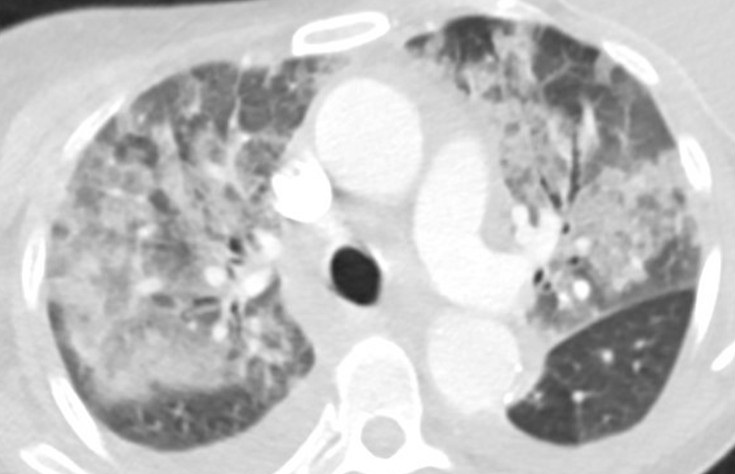
Figure 1. Axial “lung windows” reconstruction from a contrast-enhanced CT angiogram demonstrating mixed interstitial and airspace opacities consisting of smooth septal lines with patchy superimposed consolidation and ground glass with a central distribution (peripheral sparing). There are also small layering pleural effusions. Findings are nonspecific but would be considered consistent with “batwing edema” in the setting of severe alveolar edema given the clinical context. To view Figure 1 in a separate, enlarged window click here.
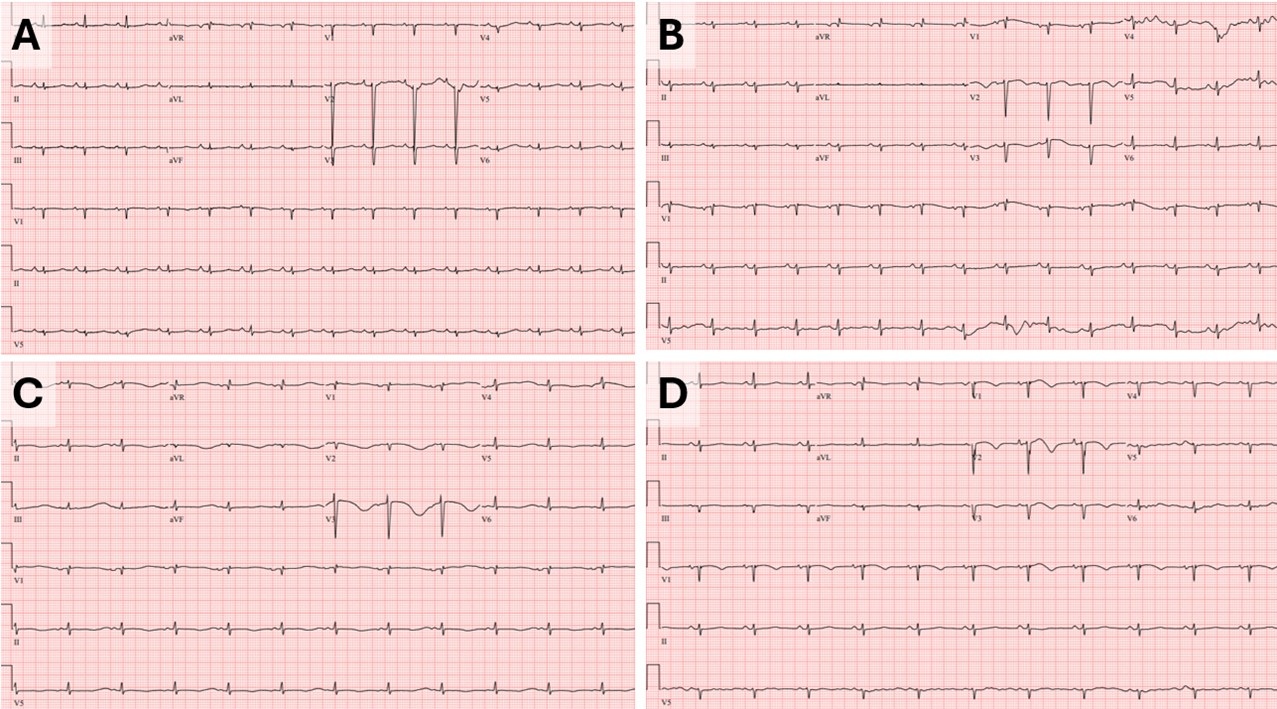
 Figure 2. Baseline ECG (A) performed 2 months prior to tips procedure: HR 90bpm, QTC 513ms. Admission ECG (B): HR 88, QTC 568ms. ECG a few hours prior to episode of V-tach (C): HR 70, QTC 726ms. ECG prior to extubation (D): HR 68, QTc 523ms. To view Figure 2 in a separate, enlarged window click here.
Figure 2. Baseline ECG (A) performed 2 months prior to tips procedure: HR 90bpm, QTC 513ms. Admission ECG (B): HR 88, QTC 568ms. ECG a few hours prior to episode of V-tach (C): HR 70, QTC 726ms. ECG prior to extubation (D): HR 68, QTc 523ms. To view Figure 2 in a separate, enlarged window click here.
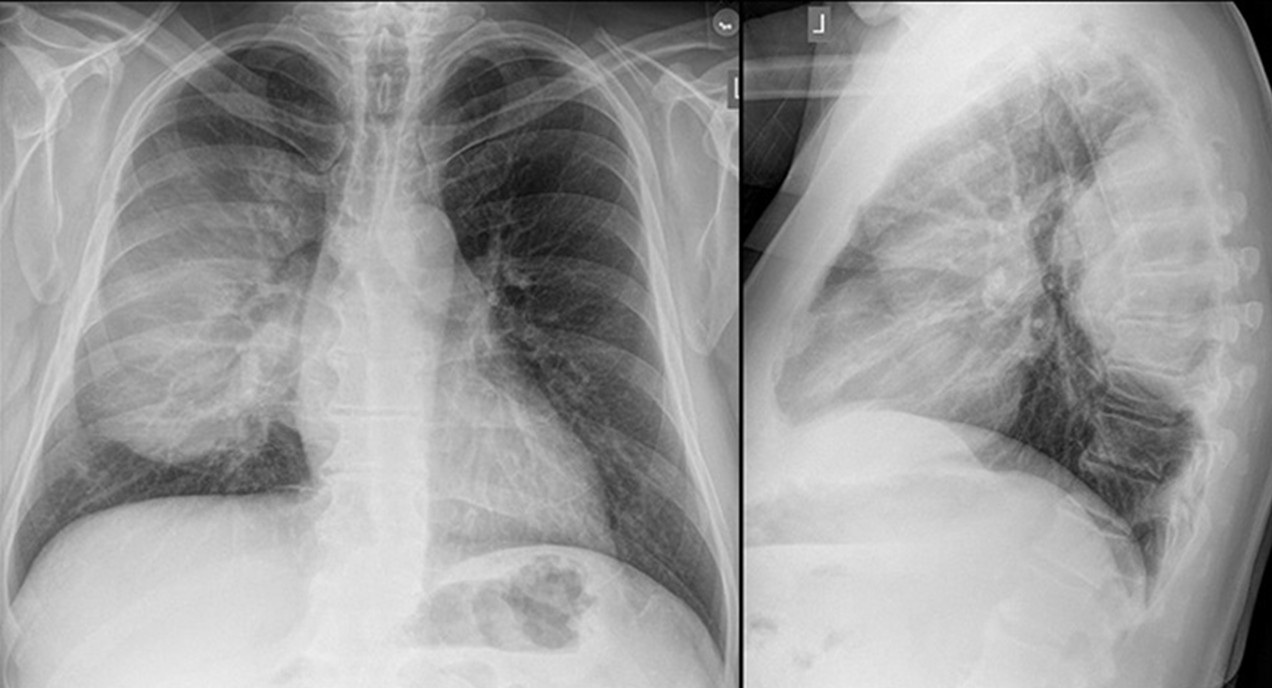
A 55-year-old woman with cirrhosis secondary to alcohol use disorder presented to the emergency department with worsening shortness of breath, orthopnea, and two recent syncopal episodes with seizure-like activity. She had undergone a transjugular intrahepatic portosystemic shunt (TIPS) procedure for refractory ascites one month prior. On arrival, she was hemodynamically stable but tachypneic (respiratory rate 22 bpm) with an SpO2 of 90% on room air. Her jugular venous pressure (JVP) was elevated. Chest X-ray showed bilateral pulmonary infiltrates. CT angiography (Figure 1) revealed bilateral patchy airspace disease with a central distribution and pleural effusions, suggesting alveolar edema. Abdominal imaging confirmed liver disease, ascites, and a TIPS. Laboratory tests revealed negative respiratory viral and SARS-CoV-2 PCR tests, ammonia was normal, BNP of 427 pg/mL, normal troponins, sodium 138 mmol/L, potassium 3.7 mmol/L, and procalcitonin 0.23 ng/mL. Blood and sputum cultures were collected. An electrocardiogram (ECG, figure-2B) showed sinus rhythm with QTc of 568 ms (baseline EKG Figure-2A). The patient was admitted to the step-down unit and started on broad-spectrum antibiotics for presumed pneumonia.
The following day she continued to have shortness of breath and also developed nausea, for which ondansetron 4 mg IV was ordered. She also received hydroxyzine which is a regular home medication. Shortly after, she developed supraventricular tachycardia (SVT) at 200 bpm, unresponsive to adenosine but controlled with 5 mg of metoprolol. Two hours later, she developed polymorphic ventricular tachycardia (V-tach) which led to cardiac arrest. After two minutes of cardiopulmonary resuscitation (CPR), spontaneous circulation was restored, and the patient was intubated and transferred to the ICU. Repeat ECG (Figure-2C) following cardiac arrest showed a prolonged QTc interval of 726 ms. In the ICU, she was sedated with a midazolam drip and diuresed with furosemide. She received magnesium and potassium replacement. Potential QT-prolonging medications were discontinued, and she was started on metoprolol 12.5 mg twice daily. Her QTc improved to 523 ms (figure-2D). Chest X-ray showed significant improvement over 24 hours, and a repeat echocardiogram showed normal ejection fraction. The patient was extubated and transferred back to the medical floor for further care. A PharmD team reviewed her medications before discharge, and she was educated on avoiding QT-prolonging drugs.
The liver is crucial in drug metabolism, primarily through the cytochrome P450 enzyme system, accounting for 40-50% of its activity. In cirrhotic patients, this activity is markedly reduced, impairing drug clearance and leading to the accumulation of QT-prolonging drugs. Additionally, cirrhotic patients have diminished intestinal CYP3A4 activity (approximately 30-40% of normal) (1). The QT interval is often prolonged in patients with both non-cirrhotic and cirrhotic portal hypertension, and portal decompression through TIPS exacerbates this abnormality (2). Furthermore, the intravenous route translates to faster drug bioavailability and higher peak blood concentrations compared to oral administration. Although this phenomenon has not been extensively studied in cirrhotic patients, it has been evaluated in emergency department patients receiving intravenous ondansetron (3). The presence of a TIPS may prolong the drug half-life, potentially increasing the risk of severe arrhythmias, such as torsades de pointes. This might explain the onset and the timing of life-threatening arrhythmias observed in our patient following the administration of intravenous ondansetron and oral hydroxyzine. In retrospect, the syncopal episodes observed at home in our case likely indicated episodes of ventricular tachycardia. Our patient had no prior history of similar events before undergoing the TIPS procedure. The combination of impaired liver function, metabolic disturbances, and the addition of a TIPS creates a "perfect storm" for life-threatening arrhythmias, particularly in those who are already on QT-prolonging medication.
Late onset pulmonary edema is another atypical presentation our case. Following a TIPS procedure, JVP may not reliably reflect the patient's true fluid status or heart function. An improvement in central hypovolemia could be attributed to an increase in thoracic blood volume, encompassing both central venous and arterial components. This is further reinforced by an increase in preload and a simultaneous decrease in afterload (4). Chronic liver disease with portal hypertension is associated with increased cardiac output, reduced peripheral vascular resistance, and normal cardiac filling pressures. Studies by Azoulay et al. (5) suggest that after the creation of a portosystemic shunt during TIPS, cardiac filling pressures rise, and a hyperdynamic cardiac state may persist for up to a month, increasing the risk of pulmonary edema. While pulmonary edema is typically an early complication post-TIPS (6), our case presented a delayed onset, which, to our knowledge, has not been previously described.
This case highlights the importance of recognizing potential complications following TIPS, particularly QTc prolongation and delayed pulmonary edema. The risk of severe QTc prolongation is heightened when patients are exposed to QT-prolonging medications. Healthcare providers should be aware of these risks and closely monitor for such life-threatening complications post TIPS.
Abdulmonam Ali, MD
SSM Health
Mount Vernon, IL USA
References
- Vuppalanchi R, Juluri R, Ghabril M, Kim S, Thong N, Gorski JC, Chalasani N, Hall SD. Drug-induced QT prolongation in cirrhotic patients with transjugular intrahepatic portosystemic shunt. J Clin Gastroenterol. 2011 Aug;45(7):638-42. [CrossRef] [PubMed]
- Trevisani F, Merli M, Savelli F, Valeriano V, Zambruni A, Riggio O, Caraceni P, Domenicali M, Bernardi M. QT interval in patients with non-cirrhotic portal hypertension and in cirrhotic patients treated with transjugular intrahepatic porto-systemic shunt. J Hepatol. 2003 Apr;38(4):461-7. [CrossRef] [PubMed]
- Rezaei Zadeh Rukerd M, Shahrbabaki FR, Movahedi M, Honarmand A, Pourzand P, Mirafzal A. Single intravenous dose ondansetron induces QT prolongation in adult emergency department patients: a prospective observational study. Int J Emerg Med. 2024 Apr 2;17(1):49. [CrossRef] [PubMed]
- Busk TM, Bendtsen F, Poulsen JH, et al. Transjugular intrahepatic portosystemic shunt: impact on systemic hemodynamics and renal and cardiac function in patients with cirrhosis. Am J Physiol Gastrointest Liver Physiol. 2018 Feb 1;314(2):G275-G286. [CrossRef] [PubMed]
- Azoulay D, Castaing D, Dennison A, Martino W, Eyraud D, Bismuth H. Transjugular intrahepatic portosystemic shunt worsens the hyperdynamic circulatory state of the cirrhotic patient: preliminary report of a prospective study. Hepatology. 1994 Jan;19(1):129-32. [PubMed]
- Willoughby PH, Beers RA, Murphy KD. Pulmonary edema after transjugular intrahepatic portosystemic shunt. Anesth Analg. 1996 Apr;82(4):895-6. [CrossRef] [PubMed]
 Post a Comment
Post a Comment
{kind=link}
{kind=link}
{kind=link}