
Medical Image of the Week: Arachnoid Cyst
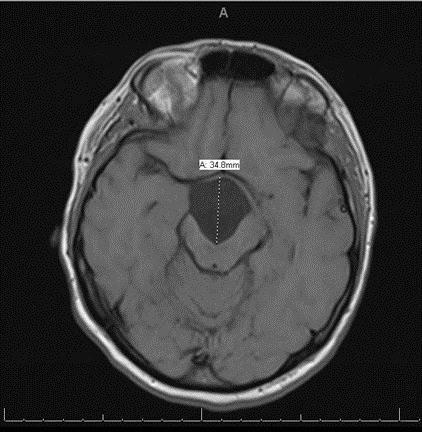
Figure 1. Axial T1 MRI of mass.

Figure 2. Coronal T2 weighted MRI demonstrating compressions onto mesial temporal lobes and stretching of the optic chiasm and tracts; upward displacement of the hypothalamus, third ventricle small in caliber and mild posterior displacement of the midbrain.
A 40 year-old woman with adult attention deficit hyperactive and bipolar 1 disorder presents with an altered mental status. Per her family, she had been non-verbal, with reduced oral intake, confusion and sedated for the past three days. Per her husband, she had episodes of diarrhea and abdominal discomfort. She was on multiple medications including ramelteon 8mg nightly, atomoxetine 40mg daily, hydroxyzine 25mg twice daily, bupropion 75mg twice daily and risperidone 2mg daily with recent addition of lithium ER 1200mg/daily started one month prior to presentation with unknown adherence.
Upon arrival, vital signs were within normal limits. Physical exam revealed an overweight Caucasian woman with a significant coarse tremor visible at rest, restlessness and diaphoresis. Neurological examination was limited by patient hesitancy, however, it did not demonstrate focal deficits except for altered consciousness with Glasgow Coma Scale of 10. Notable laboratory findings were Na+ 134 mEq/L, K+ 3.2 mEq/L, and lithium level of 3.9 mmol/L, urine toxicology positive for cocaine, and EKG showed QT prolongation. Toxicology and psychiatry were consulted.
CT of her head without contrast showed a large midline lesion in the sellar/suprasellar estimated to be 5.2x 2.1x 3.2cm. On hospital day number 2 the patient was more somnolent with down trending lithium level of 2.6 mmol/L. Later that day the patient had an observed generalized tonic clonic seizure which required abortive therapy with lorazepam and levetiracetam. A MRI revealed large arachnoid cyst measuring 3.6x3.1x3.5cm causing mass effect on adjacent tissue. (Figures 1 and 2). Neurology was consulted and recommended neurosurgery evaluation who deferred intervention to an outpatient basis given her lithium overdose as a more likely etiology of her seizure and not the arachnoid cyst.
Arachnoid cysts are cerebral spinal fluid filled sacs located between the brain or spinal cord and the arachnoid membrane. They can be either primary, which are present at birth due to developmental abnormalities of the brain and spinal cord, or they may be secondary, which are the result of head injury, meningitis, tumors, or a complication of brain surgery. Symptoms are based on the size and location of the cyst and include headache, nausea and vomiting, seizures, hearing and visual disturbances, vertigo, and difficulties with balance and walking. If the cyst compresses the spinal cord or nerve roots, then individual may experience progressive back and leg pain and tingling or numbness in the legs or arms.
Diagnosis is usually via MRI which distinguishes between fluid-filled arachnoid cysts from other types of cysts. The treatment depends on the location and the size of the cyst. If the cyst is small and does not compress any of the surrounding structures, with an absence of symptoms, no treatment is necessary. The two main ways of treating symptomatic cysts include surgery or placing a permanent shunt to drain the fluid. Surgical approaches include microscopic open surgical fenestration procedure in which the neurosurgeon opens the skull to gain access to the cyst, then opens the cyst to release pressure, allowing contents to be absorbed by the brain. Another surgical approach involves endoscopic cyst fenestration in which an endoscope is used to drain the cyst internally without having to perform an open surgery. In some instances, formal craniotomy with excision/marsupialization of the cyst into the subarachnoid space is performed. The procedure performed depends on the surgeon’s comfort with the technique and the size/location of the cyst.
Matthew Erisman MD, Rozina Parbtani MS IV, and Faraz Jaffer MD.
Department of Internal Medicine
University of Arizona at South Campus
Tucson, Arizona USA
References
- Al-Holou WN, Terman S, Kilburg C, Garton HJ, Muraszko KM, Maher CO. Prevalence and natural history of arachnoid cysts in adults. J Neurosurg. 2013 Feb;118(2):222-31. [CrossRef] [PubMed]
- Eidlitz-Markus T, Zeharia A, Cohen YH, Konen O. Characteristics and management of arachnoid cyst in the pediatric headache clinic setting. Headache. 2014 Nov-Dec;54(10):1583-90. [CrossRef] [PubMed]
Cite as: Erisman M, Parbtani R, Jaffer F. Medical image of the week: arachnoid cyst. Southwest J Pulm Crit Care. 2016;13(4):181-3. doi: http://dx.doi.org/10.13175/swjpcc074-16 PDF
 Post a Comment
Post a Comment
Reader Comments