
Medical Image of the Week: Pancoast Tumor
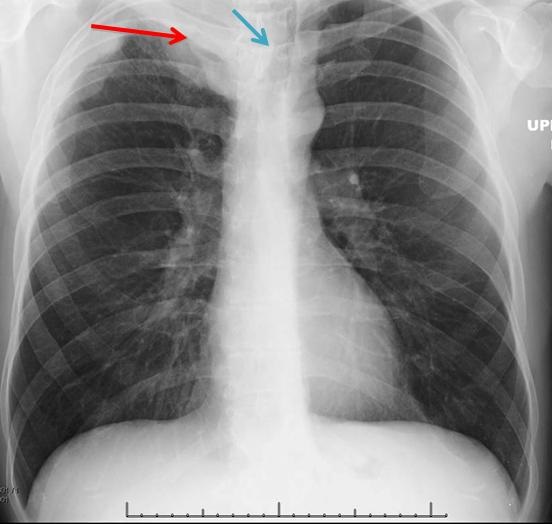
Figure 1. Chest radiograph demonstrating pleural and parenchymal mass in the right lung apex (red arrow) with tracheal deviation to the left (blue arrow).
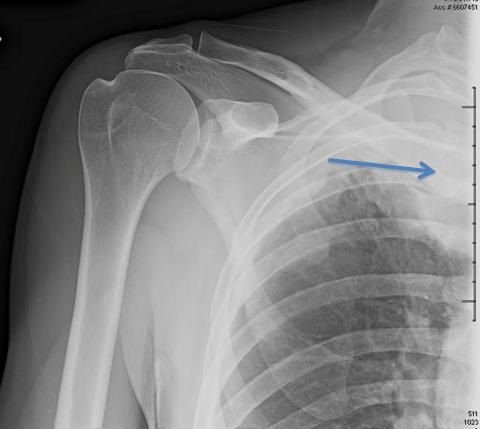
Figure 2. Right shoulder radiograph demonstrating the apical mass (blue arrow).
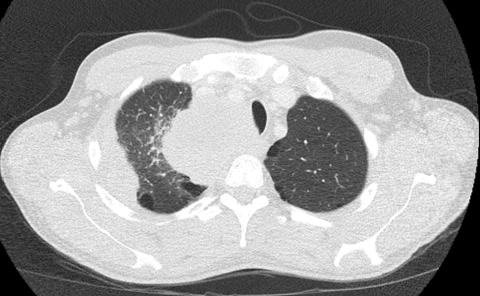
Figure 3. Chest CT (axial image) demonstrating a large mass in the right lung apex with tracheal deviation to the left.
A 39 year-old man presented to the Emergency Department with right shoulder, back and abdominal pain. He had no significant medical problems except for a 20 pack-year history of smoking. Laboratory work and an abdominal ultrasound were unremarkable and he was discharged. Approximately one week later he returned to the Emergency Department with persistent right shoulder and back pain and mild numbness and tingling of the second, third and fourth digits of his right hand. He also described weakness of his right upper eyelid and noticed he was sweating only on the left side of his face. On physical exam, anisocoria was noted with the right pupil being smaller than the left pupil.
A chest x-ray and right shoulder x-ray revealed extensive pleural and parenchymal mass in the right apex and tracheal deviation to the left (Figures 1 and 2). A CT chest with contrast showed findings consistent with extensive Pancoast neoplasm in right upper lobe, left tracheal deviation, and partial destruction of right first rib and transverse process of first dorsal vertebral body, with evidence of extension into right lower neck (Figure 3). An MRI revealed widespread metastatic disease of the spine with right-sided T10 intraspinal extradural neoplasm causing severe thoracic spinal cord compression. He underwent surgical decompression. Biopsy of the lung lesion revealed poorly differentiated sarcomatoid carcinoma. The patient received chemotherapy with doxorubicin and ifosfamide and radiation to the right lung, cervical and thoracic spine.
Pancoast’s syndrome includes Horner’s syndrome (ptosis, miosis and anhidrosis), upper extremity pain, and atrophy of the hand muscles. These symptoms result from an apical thoracic mass, most commonly a bronchogenic carcinoma that invades into the thoracic inlet and causes destruction of the cervical sympathetic nerves and brachial plexus (1). Shoulder pain is the most common initial symptom and patients may receive treatment for osteoarthritis or bursitis resulting in delay in diagnosis. While malignancy is the most common cause, infectious etiologies are an important consideration as well. A recent review documented 31 cases of Pancoast’s syndrome secondary to a variety of infectious causes including bacterial, fungal, mycobacterial and parasitic organisms (2).
Emily Des Champs MS, ACNP-BC, ACHPN, CCRN1 and Linda Snyder MD2
1Department of Medicine, Geriatrics, Palliative and General Medicine, Banner University Medical Center-Tucson
2Department of Medicine, Pulmonary, Critical Care and Palliative Medicine, Banner University Medical Center-Tucson
References
- Glassman LR, Hyman K. Pancoast tumor: a modern perspective on an old problem. Curr Opin Pulm Med. 2013;19:340-3. [CrossRef] [PubMed]
- White HD, White BA, Boethel C, Arroliga AC. Pancoast's syndrome secondary to infectious etiologies: a not so uncommon occurrence. Am J Med Sci. 2011;341(4):333-6. [CrossRef] [PubMed]
Reference as: Des Champs E, Snyder L. Medical image of the week: Pancoast tumor. Southwest J Pulm Crit Care. 2015;11(2):82-3. doi: http://dx.doi.org/10.13175/swjpcc069-15 PDF
 1 Comment
1 Comment
Reader Comments (1)
I agree A 39 year-old man presented to the Emergency Department with right shoulder, back and abdominal pain. He had no significant medical problems except for a 20 pack-year history of smoking. Laboratory work and an abdominal ultrasound were unremarkable and he was discharged