
Medical Image of the Week: Esophageal Perforation
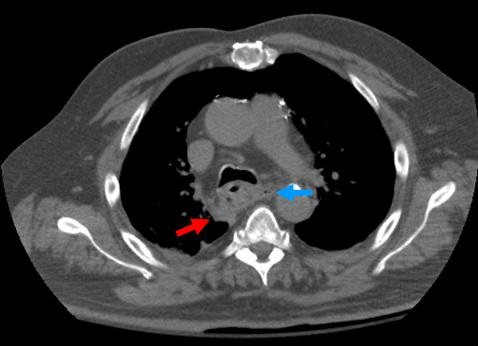
Figure 1. Axial, non-contrast CT of chest demonstrates wall thickening of the mid-thoracic esophagus with an extra-luminal focus of gas (blue arrow) in the mediastinum in addition to a small amount of right peri-esophageal fluid (red arrow).
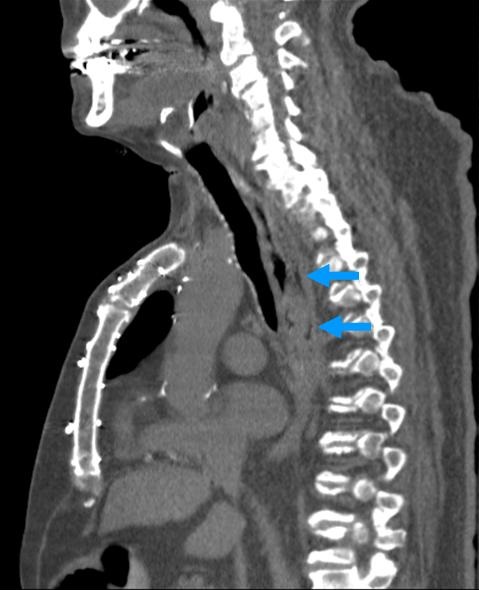
Figure 2. Sagittal, non-contrast CT of chest demonstrates extra-luminal air posterior to the mid-thoracic esophagus (blue arrows).
A 74 year old man with a past medical history of esophageal strictures status post dilatation, coronary artery disease status post CABG, and atrial fibrillation presented to hospital with complaints of severe chest pain that began after the consumption of tortilla chips one hour prior to presentation. Electrocardiogram and cardiac enzymes were not consistent with acute coronary syndrome. Chest X-ray was consistent with a widened mediastinal silhouette. Contrast esophogram was negative for extra luminal extravasation. CT scan of the chest with oral contrast demonstrated thickening of the mid-thoracic esophagus with an extra-luminal focus of gas in the mediastinum along with fluid along the inferior aspect of the esophagus (Figures 1 and 2). These findings were concerning for esophageal perforation. The patient was taken to the operating room for endoscopy which showed micro perforation in mid-esophagus.
Esophageal perforation remains a highly morbid condition. Mortality rates are based predominantly on time of presentation and the etiology of perforation. Symptoms of esophageal perforation are non-specific and include neck or chest pain, dysphagia, odynophagia, difficulty breathing, vomiting, drooling, hematemesis, and abdominal rigidity (1) Initial diagnostic assessment includes conventional radiography, which can be normal in up to 10% of patients. Follow-up contrast esophograms are used to determine the presence and precise location of an esophageal perforation. However, false negative rates of 10% have been reported (2). CT scan of the chest or abdomen is indicated when contrast esophogram cannot be performed or all other diagnostic modalities have not been helpful in diagnosing esophageal perforation despite high clinical suspicion. Extra-luminal air in the mediastinum or surrounding the esophagus is the most reliable sign and when taken in conjunction with the clinical presentation, has 92% accuracy. Other common findings include obliteration of fat planes in the mediastinum resulting from inflammation, peri-esophageal or mediastinal fluid (92% accuracy), esophageal thickening, pleural effusions, extravasation of oral contrast material into the peri-esophageal tissues, and a tract at the site of the tear (3).
Jawad Bilal MD, David Testa MD, Irbaz bin Riaz MD and Ryan Nahapetian MD MPH
University of Arizona
Tucson, AZ
References
- Aronberg RM, Punekar SR, Adam SI, Judson BL, Mehra S, Yarbrough WG. Esophageal perforation caused by edible foreign bodies: A systematic review of the literature. Laryngoscope. 2015;125(2):371-8. [CrossRef] [PubMed]
- Bladergroen MR, Lowe JE, Postlethwait RW. Diagnosis and recommended management of esophageal perforation and rupture. Ann Thorac Surg. 1986;42(3):235-9. [CrossRef] [PubMed]
- Lee S, Mergo PJ, Ros PR. The leaking esophagus: CT patterns of esophageal rupture, perforation, and fistulization. Crit Rev Diagn Imaging. 1996;37(6):461-90. [PubMed]
Reference as: Bilal J, Testa D, Riaz I, Nahapetian R. Medical image of the week: eosphageal perforation. Southwest J Pulm Crit Care. 2015;10(4):201-2. doi: http://dx.doi.org/10.13175/swjpcc033-15 PDF
 Post a Comment
Post a Comment
Reader Comments