
Medical Image of the Week: Malignant Pericardial Effusion and Cardiac Tamponade

Figure 1. EKG showing sinus tachycardia, low QRS voltage and electric alternans, suggesting pericardial effusion.
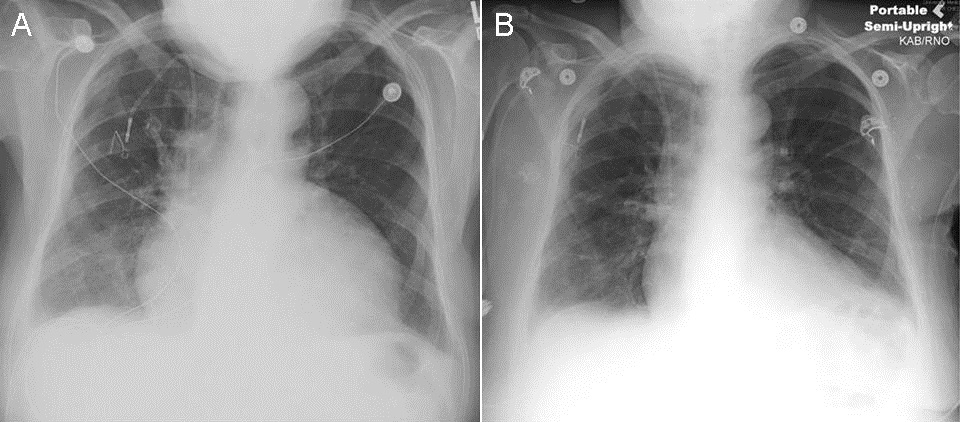
Figure 2. Chest X-ray pre- and post-pericardiocentesis. Panel A: Cardiomegaly with water bottle shape shown before procedure. Panel B: resolution after drainage of 1.8 L of pericardial fluid.

Figure 3. Echocardiogram showing massive pericardial effusion (dashed line), floating heart, and collapsed right atrium and ventricle that are consistent with cardiac tamponade.

Figure 4. Intra-pericardial space pressure tracing with maximum pressure measured at 25 mmHg.
A 53 year old woman with history of metastatic breast cancer presented to the emergency department (ED) with worsening shortness of breath for 2 weeks. She was initially diagnosed with grade III breast intraductal carcinoma was estrogen receptor, progesterone receptor, and HER2 negative 5 years earlier. A lumpectomy was performed followed by 4 cycles of chemotherapy with cyclophosphamide and taxol as well as radiation therapy. However, follow-up CT and MRI and subsequent biopsy demonstrated metastatic disease in the left adrenal gland, right ovary, and mediastinal lymph nodes, for which additional chemotherapy was started a month prior to presentation. In the ED, the patient was tachycardic and tachypneic. Vital signs showed BP 112/94 mmHg, HR 118 /min, RR 28 /min, temperature 97.5 °F, and SpO2 97 % with room air. EKG showed sinus tachycardia, low QRS voltage with electric alternans (Figure 1), and chest x-ray demonstrated cardiomegaly with a water bottle shaped heart (Figure 2A), suggesting pericardial effusion. Over the hour at ED, patient developed sudden hypotension with BP of 78/44. 1 L of normal saline was administrated immediately, and patient was transferred to cardiac catherization laboratory for emergent pericardiocentesis. Echocardiogram before the procedure demonstrated massive pericardial effusion and a floating heart in the pericardial space (Figure 3). Intra-pericardial pressure was measured at 25 mmHg (Figure 4). A total of 1.8 L of sanguineous fluid was drained. Pericardial fluid cell count with differential and chemistry showed WBC 2444 /μL, RBC 1480000 /μL, lymphocytes 32 /μL , neutrophils 64 /μL, glucose 108 mg/dL, and protein 5.2 g/dL, and cytology analysis with fluid demonstrated adenocarcinoma, confirming the diagnosis of malignant pericardial effusion and cardiac tamponade. Chest x-ray after the procedure showing resolution of the water bottle-shaped heart (Figure 2B). Elective thoracotomy with pericardiectomy was performed the next day, and patient was eventually discharged in stable condition.
Pericardial effusion seen in cancer patients may results from several sources. Constrictive pericarditis with pericardial effusion can arise as a complication of radiation therapy. Uremia and certain medications can induce pericardial effusion as well. Metastatic cardiac involvement may causes pericardial effusion. A previous autopsy study showed 10.7 % of patients with underlying malignancy had metastatic disease in the heart (1). Adenocarcinoma is the most frequently found cell type, and lung cancer, malignant lymphoma and breast cancers are the most common primary tumors metastasizing to the heart. Symptoms of malignant pericardial effusion include shortness of breath, cough, chest pain, and edema. Vaitkus et al. (2) proposed three goals in the management of symptomatic malignant pericardial effusion:1) relief of immediate symptoms, 2) determination of cause, and 3) prevention of recurrence (2). No single modality has been proved to be superior since most patients with malignant pericardial effusion need more than one therapeutic modality. Pericardiocentesis is commonly used for acute symptomatic relief while other chemical or mechanical modalities such as systemic chemotherapy, radiation therapy, intrapericardial sclerosing agents, indwelling pericardial catheter, or thoracotomy with pericardiectomy are options to prevent relapse.
Seongseok Yun, MD PhD; Juhyung Sun, BS; Rorak Hooten, MD; Yasir Khan, MD;Craig Jenkins, MD
Department of Medicine, University of Arizona, Tucson, AZ 85724, USA
References
- Klatt EC, Heitz DR. Cardiac metastases. Cancer. 1990;65(6):1456-9. [CrossRef]
- Vaitkus PT, Herrmann HC, LeWinter MM. Treatment of malignant pericardial effusion. JAMA. 1994;272(1):59-64. [CrossRef] [PubMed]
Reference as: Yun S, Sun J, Hooten R, Khan Y, Jenkins C. Medical image of the week: malignant pericardial effusion and cardiac tamponade. Southwest J Pulm Crit Care. 2014;8(6):343-6. doi: http://dx.doi.org/10.13175/swjpcc048-14 PDF
 Post a Comment
Post a Comment
Reader Comments