
Airway Registry and Training Curriculum Improve Intubation Outcomes in the Intensive Care Unit
Joshua Malo MD1
Cameron Hypes MD2
Bhupinder Natt MBBS1
Elaine Cristan MD1
Jeremy Greenberg MD1
Katelin Morrissette MD1
Linda Snyder MD1
James Knepler MD1
John Sakles MD2
Kenneth Knox MD1
Jarrod Mosier MD2
1 Department of Medicine, University of Arizona College of Medicine, Tucson, AZ
2 Department of Emergency Medicine, University of Arizona College of Medicine, Tucson, AZ
Abstract
Background: Intubation in critically ill patients remains a highly morbid procedure, and the optimal approach is unclear. We sought to improve the safety of intubation by implementing a simulation curriculum and monitoring performance with an airway registry.
Methods and Methods: This is a prospective, single-center observational study of all intubations performed by the medical intensive care unit (ICU) team over a five-year period. All fellows take part in a simulation curriculum to improve airway management performance and minimize complications. An airway registry form is completed immediately after each intubation to capture relevant patient, operator, and procedural data.
Results: Over a five-year period, the medical ICU team performed 1411 intubations. From Year 1 to Year 5, there were significant increases in first-attempt success (72.6 vs. 88.0%, p<0.001), use of video laryngoscopy (72.3 vs. 93.5%, p<0.001), and use of neuromuscular blocking agents (73.5 vs. 88.4%, p<0.001). There were concurrent decreases in rates of desaturation (25.6 vs. 17.1%, p=0.01) and esophageal intubations (5 vs. 1%, p=0.009). Low rates of hypotension (8.3%) and cardiac arrest (0.6%) were also observed.
Conclusions: The safety of intubation in critically ill patients can be markedly improved through joint implementation of an airway registry and simulation curriculum.
Introduction
Airway management is one of the highest risk procedures that can be performed in the intensive care unit (ICU). Despite technologic advances in methods for performing intubation, recent studies continue to report frequent adverse events associated with tracheal intubation, and complications occur in up to 40% of procedures (1-3). Even in the absence of anatomic predictors of a difficult airway, critically ill patients are particularly vulnerable to desaturation, hemodynamic instability, and cardiac arrest due to poor physiologic reserve (4, 5). Repeated or prolonged intubation attempts exhaust any physiologic reserve these patients may have, leading to more frequent adverse outcomes (6). Thus, maximizing first attempt success without an adverse event is the goal for airway management in this high-risk population (7, 8).
Much of the clinical practice regarding airway management in the ICU has been extrapolated from studies performed during elective intubations in the operating room (4). In recent years, there has been a greater focus on management strategies and outcomes in critically ill patients in the emergency department (ED) and ICU (3, 9, 10). In 2012, we initiated a comprehensive airway management quality improvement program to measure variables related to airway management in the ICU and identify targeted opportunities for intervention to improve outcomes (11). We first established a prospectively collected registry of all intubations performed in the medical ICU. After evaluation of the first year of data, a simulation-based curriculum for the pulmonary and critical care fellows was developed with a focus on identifying high-risk features, minimizing adverse events, and maximizing first-attempt success. Lastly, research questions were evaluated periodically to identify targeted opportunities for improvement. This paper will describe the outcomes after the first 5 years of our program.
Materials and Methods
This is a prospective single-center observational study of all intubations performed in the medical ICU from January 1, 2012 to December 31, 2016. The study has been granted an exemption from full review and is approved by the University of Arizona Institutional Review Board. The primary outcome of interest was first attempt success, while secondary outcomes included adverse events, drug and device selection, and method of preoxygenation.
This study took place at a large academic medical center with 20+ bed medical ICU. A medical ICU team consisting of an attending intensivist, a pulmonary/critical care or emergency medicine/critical care fellow, and internal medicine, emergency medicine, and occasionally family medicine residents assumes primary management of all patients admitted to the medical ICU service. All patients admitted to the ICU undergoing airway management by the medical ICU team were included in the study.
We have maintained a continuous quality improvement (CQI) database for all episodes of airway management performed by our medical intensive care teams since January 1, 2012. After each intubation, the operators record data pertinent to the procedure, including difficult airway characteristics, drug and device selection, and number of attempts, using a standardized form. The study primary investigator crosschecked a report generated by the electronic health record against the database to ensure forms were completed for all intubations. Forms were reviewed for completeness and internal consistency. Inconsistent or absent data were resolved by interview of the operator. The variables captured in the form have been previously described (11) and are adjusted occasionally to evaluate new variables of interest.
Our Pulmonary and Critical Care Medicine (PCCM) and Critical Care Medicine (CCM) fellowship programs implemented an 11-month, simulation-based airway management curriculum beginning on July 1, 2013. The curriculum is designed to improve situational awareness in the peri-intubation period as well as to emphasize techniques that will optimize chances of first-attempt success while minimizing complications. The general outline for the simulations has been previously described in detail (11). Briefly, the curriculum involves clinical scenarios of varying and generally progressive complexity, each of which is meant to emphasize certain aspects of airway management. As trainees progress, the curriculum emphasizes the identification and mitigation of factors that may decrease the likelihood of first-attempt success and increase the likelihood of complications. The annual fellowship complement includes 14 Pulmonary and Critical Care Medicine fellows and 2 Critical Care Medicine fellows. All fellows participate in the curriculum, which is updated to include recent advances in airway management from the literature and analysis of our own airway registry. A debriefing session following each simulation is used to emphasize specific learning points for the approach to airway management.
Statistical Analysis
Descriptive statistics were calculated for measured variables as means and standard deviations, medians and interquartile ranges (IQR), or proportions as appropriate. Categorical variables were compared using Fisher’s exact test. Comparisons between Year 1 and Year 5 were performed using the Two-Sample Test of Proportions. Categorical variables with multiple groups, such as preoxygenation, Operator PGY, and Device were evaluated with the test for trend using the likelihood ratio test. All statistical analyses were performed with Stata Version 14 (StataCorp, College Station, TX).
Results
During the 60-month study period, there were 1411 intubations performed. The patient and operator characteristics are shown in Table 1 and Table 2, respectively.
Table 1. Patient characteristics.
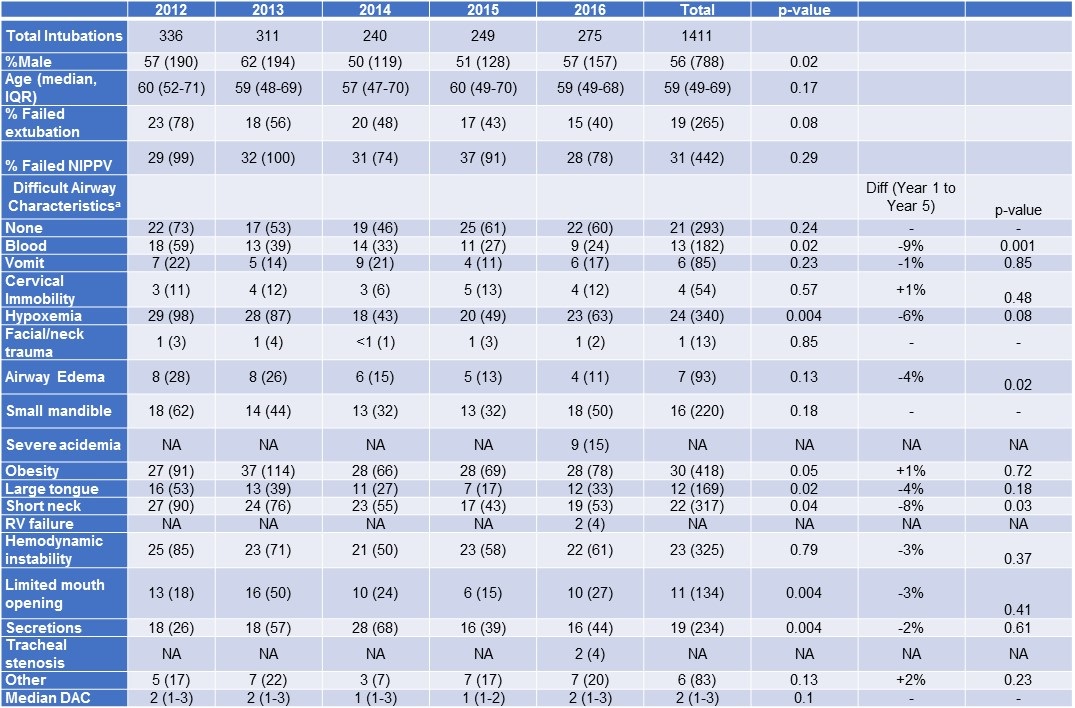
aSome DACs added over time. Limited mouth opening and secretions added after the first 8 months of data collection.
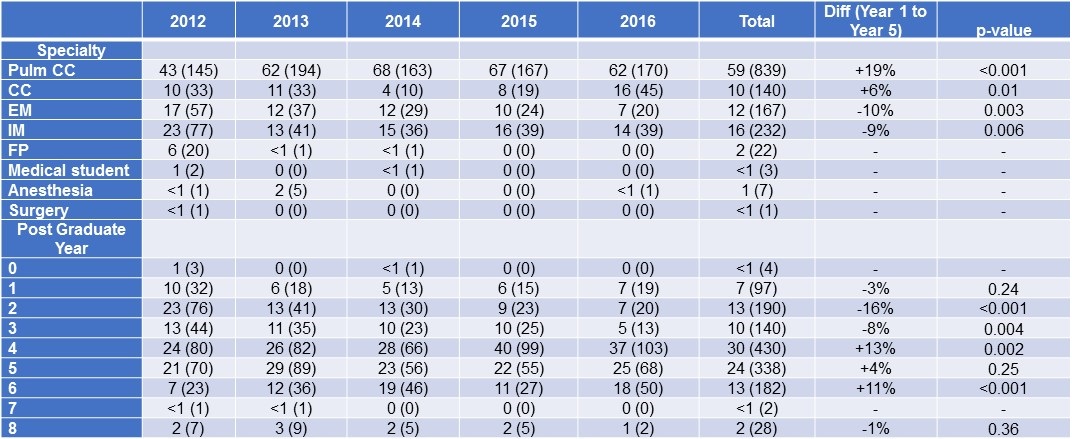
Table 2. First Operator Characteristics.
During the course of the study, there was no significant change in patient age or gender, the presence of difficult airway characteristics, starting saturation, or percentage of patients intubated after failing noninvasive positive pressure ventilation (NIPPV). There was a trend for decreased intubations resulting from failed extubation. The overall characteristics of intubation attempts are described in Table 3.
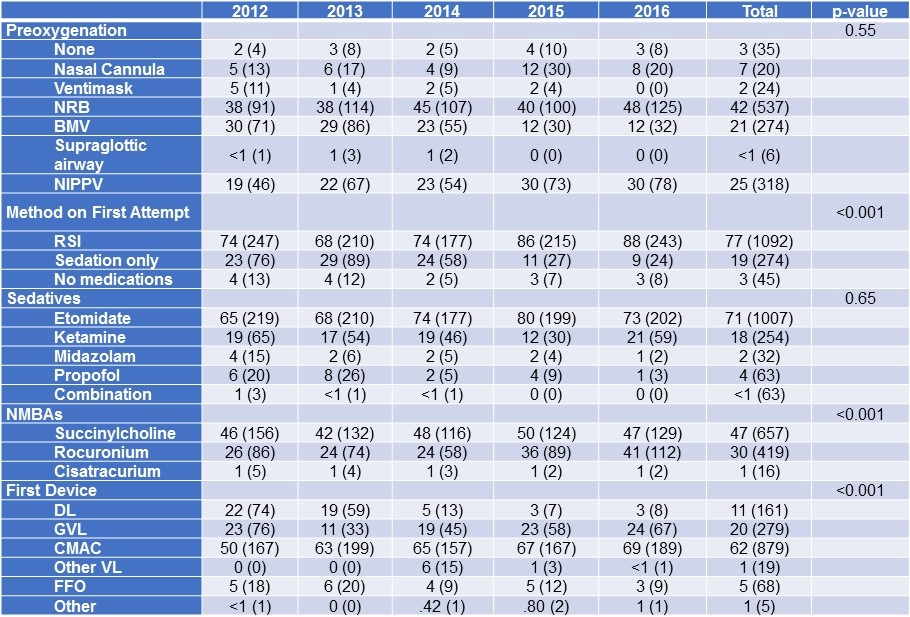
Table 3. Intubation characteristics.
There was a significant increase in the number of intubations performed by PCCM operators after the first year of the study (Year 1-5 difference +19%, p<0.001) accompanied by a decrease in intubations performed by internal medicine (Year 1-5 difference -9%, p=0.006) and emergency medicine residents (Year 1-5 difference -10%, p=0.003). Likewise, there was an increase in intubations performed by PGY 4 (Year 1-5 difference +13%, p=0.002) and PGY 6 (Year 1-5 difference +11%, p<0.001) operators with a concurrent decrease in those performed by PGY 2 (Year 1-5 difference -16%, p<0.001) and PGY 3 (Year 1-5 difference -8%, p=0.004) operators.
First-attempt success (FAS) occurred in 80.7% of intubations performed during the study period. The FAS rate increased linearly throughout the study period, with FAS of 72.6% in the first year and 88.0 % in the final year when looking at all operators (p<0.001) (Table 4, Figure 1, next page).
There was a significant increase in the number of intubations performed by PCCM operators after the first year of the study (Year 1-5 difference +19%, p<0.001) accompanied by a decrease in intubations performed by internal medicine (Year 1-5 difference -9%, p=0.006) and emergency medicine residents (Year 1-5 difference -10%, p=0.003). Likewise, there was an increase in intubations performed by PGY 4 (Year 1-5 difference +13%, p=0.002) and PGY 6 (Year 1-5 difference +11%, p<0.001) operators with a concurrent decrease in those performed by PGY 2 (Year 1-5 difference -16%, p<0.001) and PGY 3 (Year 1-5 difference -8%, p=0.004) operators.
First-attempt success (FAS) occurred in 80.7% of intubations performed during the study period. The FAS rate increased linearly throughout the study period, with FAS of 72.6% in the first year and 88.0 % in the final year when looking at all operators (p<0.001) (Table 4, Figure 1).
Table 4. Outcomes.
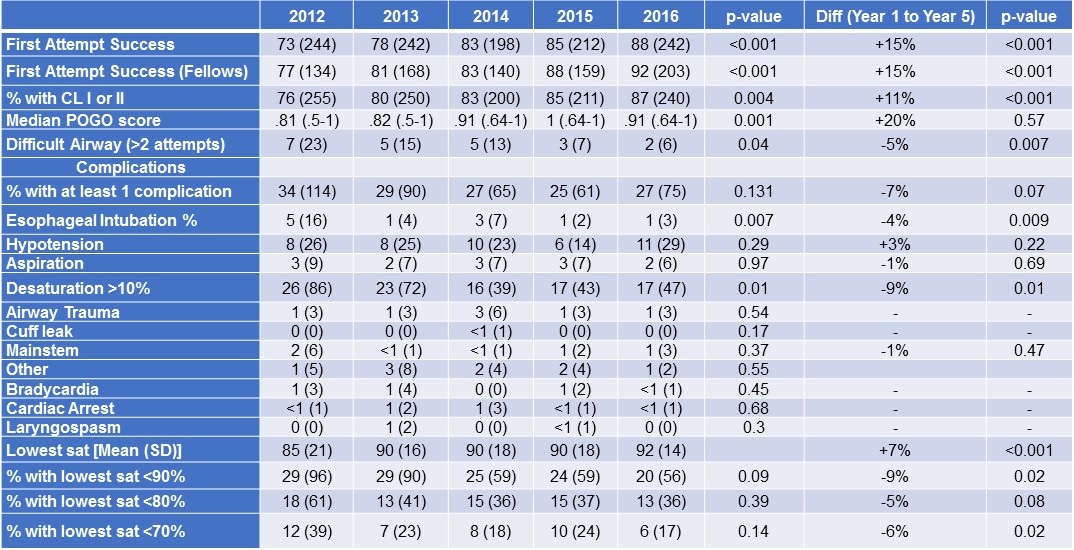
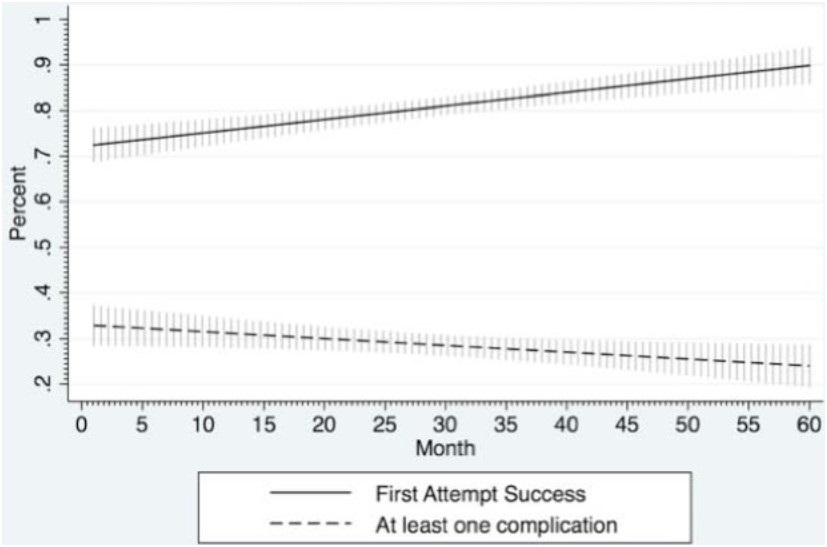
Figure 1. First-attempt success and complications over time.
For patients intubated by fellows only, FAS increased from 77% to 92% over the 5-year period (p<0.001).
During the entire study period, at least one complication occurred in 28.7% of intubations. The incidence of complications decreased throughout the first 48 months but increased slightly in the final 12 months of the study, driven primarily by an increase in hypotension (Table 4, Figure 2).
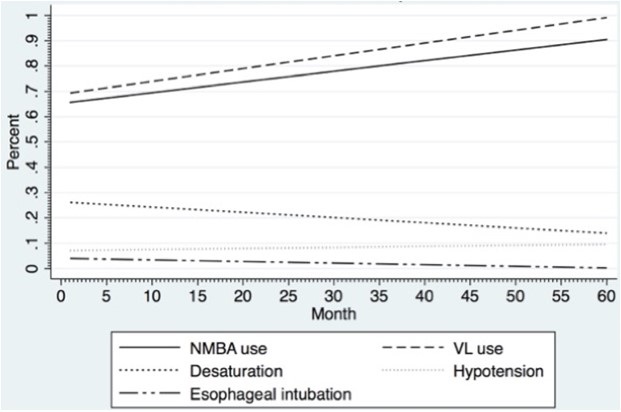
Figure 2. Neuromuscular blocking agent (NMBA) use, video laryngoscopy (VL) use, and occurrence of esophageal intubations, desaturation, and hypotension over time.
There was a decrease in the rate of desaturation from the first year to the final year of the study (25.6% to 17.1%, p=0.01). Esophageal intubations also decreased significantly over this time (5% to 1%, p=0.009). Hypotension and cardiac arrest occurred in 8.3% and 0.6% of intubations, respectively, during the entire study period.
There was a trend towards decreased use of midazolam and propofol throughout the study period while the use of etomidate tended to increase, although these changes were not significant (Table 3). A neuromuscular blocking agent (NMBA) was used in 77.4% of intubations during the study period, increasing from the first year to the final year (73.5% to 88.4%, p<0.001), driven primarily by an increase in the use of rocuronium.
There was a significant transition from the use of direct laryngoscopy (DL) to video laryngoscopy (VL) over the course of the study (p<0.001). DL was chosen as the first approach in 22.0% of intubations in the first year and only 2.9% in the final year. Conversely, the use any form of VL on the first attempt increased from 72.3% of intubations in the first year to 93.5% in the final year. Flexible fiber optic intubation was used infrequently during the entire study period, being the first device used in 4.3% of intubations.
Various methods of preoxygenation were used throughout the study period with some form of preoxygenation occurring in 97.5% of intubations. From the first year to the final year of the study, the use of bag-valve-mask (BVM) ventilation tended to decrease (30% to 12.2%) with a concurrent trend in increasing use of NIPPV for preoxygenation (19.4% to 29.7%).
Discussion
Our experience demonstrates that utilization of a comprehensive approach to airway management including an ongoing simulation-based training curriculum and CQI database is associated with an improved first-attempt success rate for the intubation of critically ill patients. This was accompanied by changes in approach to airway management, with increased use of VL and NMBA on the first attempt, as well as an increased proportion of airways being managed by more experienced operators.
While some of the observed improvement in FAS may be attributed to more experienced operators managing the airway on the first attempt, the sharp increase in fellow-level operators after implementation of the curriculum may point to increased fellow confidence or increased recognition of high-risk patients. Furthermore, as adjunctive strategies such as ramp positioning (12-14) and apneic oxygenation (15, 16) have become increasingly recognized as potentially beneficial, a continuous training curriculum provides opportunities for evaluating trainees’ knowledge of these techniques and reinforcing their incorporation into airway management.
We have previously reported on the impact of a simulation-based curriculum on operator confidence, first-attempt success, and procedural complications (11). The combination of this curriculum with a CQI database has a marked effect on the approach to management of these patients. Strategies presented and employed in the curriculum have been informed by previous reports from our database. For example, after demonstrating improved first-attempt success with the use of neuromuscular blockade (17) and video laryngoscopy (18), the didactic portion of our curriculum incorporated these findings, which were rapidly used with increasing frequency in our intensive care unit. The integration of the curriculum and CQI database facilitates adoption of best practices, leading to a significant improvement of first-attempt success rate over a relatively short time span. The continued improvement over the course of five years is likely due to the incorporation of the practices above during this time.
Tools traditionally used for predicting difficulty of airway management have focused primarily on characteristics of an anatomically difficult intubation (19, 20). More recently, there has been an expanded focus on physiologic characteristics that may lead to complications and decreased success of intubation. However, currently available instruments for ICU patients, such as the MACOCHA score, continue to put heavy emphasis on anatomic factors and are not validated for the use of VL (21). We have found difficult airway characteristics associated with decreased FAS in the setting of VL and have focused efforts at minimizing their impact (22). In our population, we noted a consistent improvement in Cormack-Lehane grade and percentage of glottic opening (POGO) score, despite a high prevalence of anatomic difficult airway characteristics. We have also noted a significant decrease in desaturations, esophageal intubations, and a trend towards decreased overall complications. In comparison to other studies of intubation complications in critically ill patients, we found generally lower rates of esophageal intubation (1, 2, 6) and similar (10) or lower rates of desaturation (1, 2) (Table 5).
Table 5. Incidence of complications in the published literature.
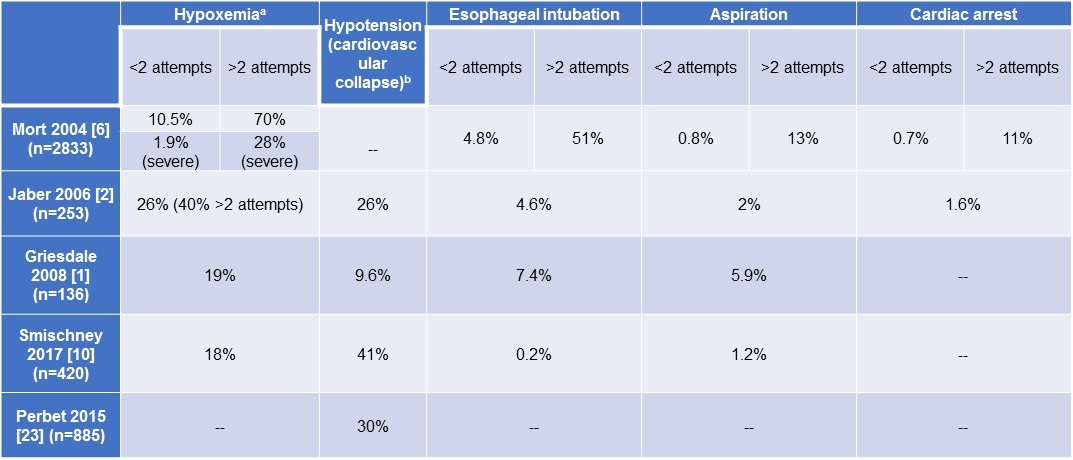
Our rate of hypotension is fairly low relative to several other studies (2, 10, 23) despite a fairly inclusive definition (administration of fluid or phenylephrine bolus, initiation or increase of vasopressor infusion). Moreover, cardiac arrest was extremely uncommon in our population, occurring in 0.57% of intubations.
Data regarding optimal approach have been controversial, and randomized trial results do not always coincide with observational studies. Although randomized controlled trials have called into question the benefit of VL (24-27), there are several important limitations to each of these studies to consider when interpreting the comparison between DL and VL. In some, patients were excluded either directly (25) or indirectly (24, 26) for a history of a difficult intubation or anticipated difficult intubation. The use of endotracheal tubes without a stylet may have also influenced outcomes (27).
Our experience is a pragmatic example of the effect of device selection on first attempt success in that we have >1400 patients, operators with varying experience, and have no patients excluded because of potential difficulty. Thus, while randomized trials may be ideal, they are costly and time-consuming and may delay identification and implementation of best practices. The FAS rate in our cohort in its first year was similar to that observed in several of these trials but improved substantially over the 5-year period. One reason for the improved FAS in our study may be the continuous simulation-based training with a focus on video laryngoscopy as the first technique of choice for the majority of airways. In comparison to other widely cited studies of airway management in critically ill patients (1, 21), our cohort demonstrated a very low incidence of difficult airways, only 2% in the final year, despite a similar presence of difficult airway characteristics. This may be an effect of the training program suggesting that perhaps airway training with a global view of airway management focusing on increasing FAS and reducing complications is even more important than equipment considerations.
Our study has several limitations. The single-center, observational nature of this study makes it at risk of bias despite attempts to identify and control for factors that may influence the results. Data forms were completed by the operator, introducing potential for reporting bias, although attempts to minimize this were made by intermittent correlation with the medical record. Although FAS is an accepted outcome for studies evaluating intubation strategies, data regarding mortality or late morbidity were not captured. The increase in hemodynamic complications in the final year is of interest, but data regarding this complication and its consequences were limited and should be a focus of future research. Despite these limitations, the consistent improvement in FAS and low incidence of difficult airways in the final year of the study warrant serious consideration of these findings.
Conclusion
We have found that a comprehensive strategy employing a simulation-based curriculum and continuous quality improvement database was associated with significant improvements in first-attempt success at intubation in critically ill patients throughout the 5-year study period. We suggest that wider adoption of this practice could vastly improve the safety of intubation in this high-risk patient population.
References
- Griesdale DE, Bosma TL, Kurth T, Isac G, Chittock DR. Complications of endotracheal intubation in the critically ill. Intensive Care Med. 2008;34(10):1835-42. [CrossRef] [PubMed]
- Jaber S, Amraoui J, Lefrant JY, Arich C, Cohendy R, Landreau L, et al. Clinical practice and risk factors for immediate complications of endotracheal intubation in the intensive care unit: a prospective, multiple-center study. Crit Care Med. 2006;34(9):2355-61. [CrossRef] [PubMed]
- Lapinsky SE. Endotracheal intubation in the ICU. Crit Care. 2015;19:258. [CrossRef] [PubMed]
- Mort TC. The incidence and risk factors for cardiac arrest during emergency tracheal intubation: a justification for incorporating the ASA Guidelines in the remote location. J Clin Anesth. 2004;16(7):508-16. [CrossRef] [PubMed]
- Mosier JM, Joshi R, Hypes C, Pacheco G, Valenzuela T, Sakles JC. The Physiologically Difficult Airway. West J Emerg Med. 2015;16(7):1109-17. [CrossRef] [PubMed]
- Mort TC. Emergency tracheal intubation: complications associated with repeated laryngoscopic attempts. Anesth Analg. 2004;99(2):607-13, table of contents. [CrossRef] [PubMed]
- Hypes C, Sakles J, Joshi R, Greenberg J, Natt B, Malo J, et al. Failure to achieve first attempt success at intubation using video laryngoscopy is associated with increased complications. Intern Emerg Med. 2017 Dec;12(8):1235-43. [CrossRef] [PubMed]
- Park L, Zeng I, Brainard A. Systematic review and meta-analysis of first-pass success rates in emergency department intubation: Creating a benchmark for emergency airway care. Emerg Med Australas. 2017;29(1):40-7. [CrossRef] [PubMed]
- Simpson GD, Ross MJ, McKeown DW, Ray DC. Tracheal intubation in the critically ill: a multi-centre national study of practice and complications. Br J Anaesth. 2012;108(5):792-9. [CrossRef] [PubMed]
- Smischney NJ, Seisa MO, Heise KJ, Busack KD, Loftsgard TO, Schroeder DR, et al. Practice of Intubation of the Critically Ill at Mayo Clinic. J Intensive Care Med. 2017:885066617691495. [CrossRef] [PubMed]
- Mosier JM, Malo J, Sakles JC, Hypes CD, Natt B, Snyder L, et al. The impact of a comprehensive airway management training program for pulmonary and critical care medicine fellows. A three-year experience. Ann Am Thorac Soc. 2015;12(4):539-48. [CrossRef] [PubMed]
- Khandelwal N, Khorsand S, Mitchell SH, Joffe AM. Head-Elevated Patient Positioning Decreases Complications of Emergent Tracheal Intubation in the Ward and Intensive Care Unit. Anesth Analg. 2016;122(4):1101-7. [CrossRef] [PubMed]
- Ramkumar V, Umesh G, Philip FA. Preoxygenation with 20 masculine head-up tilt provides longer duration of non-hypoxic apnea than conventional preoxygenation in non-obese healthy adults. J Anesth. 2011;25(2):189-94. [CrossRef] [PubMed]
- Turner JS, Ellender TJ, Okonkwo ER, Stepsis TM, Stevens AC, Sembroski EG, et al. Feasibility of upright patient positioning and intubation success rates at two academic emergency departments. Am J Emerg Med. 2017. [CrossRef] [PubMed]
- Mosier JM, Hypes CD, Sakles JC. Understanding preoxygenation and apneic oxygenation during intubation in the critically ill. Intensive Care Med. 2017;43(2):226-8. [CrossRef] [PubMed]
- Sakles JC, Mosier JM, Patanwala AE, Arcaris B, Dicken JM. First Pass Success Without Hypoxemia Is Increased With the Use of Apneic Oxygenation During Rapid Sequence Intubation in the Emergency Department. Acad Emerg Med. 2016;23(6):703-10. [CrossRef] [PubMed]
- Mosier JM, Sakles JC, Stolz U, Hypes CD, Chopra H, Malo J, et al. Neuromuscular blockade improves first-attempt success for intubation in the intensive care unit. A propensity matched analysis. Ann Am Thorac Soc. 2015;12(5):734-41. [CrossRef] [PubMed]
- Hypes CD, Stolz U, Sakles JC, Joshi RR, Natt B, Malo J, et al. Video Laryngoscopy Improves Odds of first-attempt success at intubation in the intensive care unit. A propensity-matched analysis. Ann Am Thorac Soc. 2016;13(3):382-90. [CrossRef] [PubMed]
- Mallampati SR, Gatt SP, Gugino LD, Desai SP, Waraksa B, Freiberger D, et al. A clinical sign to predict difficult tracheal intubation: a prospective study. Can Anaesth Soc J. 1985;32(4):429-34. [CrossRef] [PubMed]
- Wilson ME, Spiegelhalter D, Robertson JA, Lesser P. Predicting difficult intubation. Br J Anaesth. 1988;61(2):211-6. [CrossRef] [PubMed]
- De Jong A, Molinari N, Terzi N, Mongardon N, Arnal JM, Guitton C, et al. Early identification of patients at risk for difficult intubation in the intensive care unit: development and validation of the MACOCHA score in a multicenter cohort study. Am J Respir Crit Care Med. 2013;187(8):832-9. [CrossRef] [PubMed]
- Joshi R, Hypes CD, Greenberg J, Snyder L, Malo J, Bloom JW, et al. Difficult airway characteristics associated with first-attempt failure at intubation using video laryngoscopy in the intensive care unit. Ann Am Thorac Soc. 2017;14(3):368-75. [CrossRef] [PubMed]
- Perbet S, De Jong A, Delmas J, Futier E, Pereira B, Jaber S, et al. Incidence of and risk factors for severe cardiovascular collapse after endotracheal intubation in the ICU: a multicenter observational study. Crit Care. 2015;19:257. [CrossRef] [PubMed]
- Driver BE, Prekker ME, Moore JC, Schick AL, Reardon RF, Miner JR. Direct versus video laryngoscopy using the c-mac for tracheal intubation in the emergency department, a randomized controlled trial. Acad Emerg Med. 2016;23(4):433-9. [CrossRef] [PubMed]
- Griesdale DE, Chau A, Isac G, Ayas N, Foster D, Irwin C, et al. Video-laryngoscopy versus direct laryngoscopy in critically ill patients: a pilot randomized trial. Can J Anaesth. 2012;59(11):1032-9. [CrossRef] [PubMed]
- Janz DR, Semler MW, Lentz RJ, Matthews DT, Assad TR, Norman BC, et al. Randomized trial of video laryngoscopy for endotracheal intubation of critically ill adults. Crit Care Med. 2016;44(11):1980-7. [CrossRef] [PubMed]
- Lascarrou JB, Boisrame-Helms J, Bailly A, Le Thuaut A, Kamel T, Mercier E, et al. Video laryngoscopy vs direct laryngoscopy on successful first-pass orotracheal intubation among ICU patients: A randomized clinical trial. JAMA. 2017;317(5):483-93. [CrossRef] [PubMed]
Cite as: Malo J, Hypes C, Natt B, Cristan E, Greenberg J, Morrissette K, Snyder L, Knepler J, Sakles J, Knox K, Mosier J. Airway registry and training curriculum improve intubation outcomes in the intensive care unit. Southwest J Pulm Crit Care. 2018;16(4):212-23. doi: https://doi.org/10.13175/swjpcc037-18 PDF
 Post a Comment
Post a Comment
Reader Comments