
Ultrasound for Critical Care Physicians: Characteristic Findings in A Complicated Effusion
Emilio Perez Power MD, Madhav Chopra MD, Sooraj Kumar MD, Tammy Ojo MD, and James Knepler MD
Division of Pulmonary, Allergy, Critical Care and Sleep
University of Arizona College of Medicine
Tucson, AZ USA
Case Presentation
A 60-year-old man with right sided invasive Stage IIB squamous lung carcinoma, presented with a one week history of progressively worsening shortness of breath, fever, and chills. On admission, the patient was hemodynamically stable on 5L nasal cannula with an oxygen saturation at 90%. Physical exam was significant for a cachectic male in moderate respiratory distress using accessory muscles but able to speak in full sentences. His pulmonary exam was significant for severely reduced breath sound on the right along with dullness to percussion. His initial laboratory finding showed a mildly elevated WBC count 15.3 K/mm3, which was neutrophil predominant and initial chest x-ray with complete opacification of the right hemithorax. An ultrasound of the right chest was performed (Figure 1).
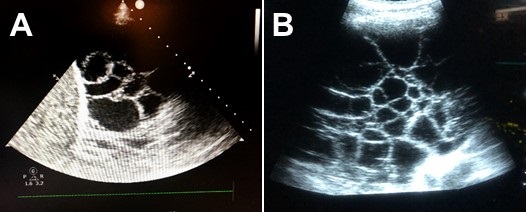
Figure 1. Ultrasound of the right chest, mid axillary line, coronal view.
Based on the ultrasound image shown what is the likely cause of the patient’s opacified right hemithorax?
Cite as: Power EP, Chopra M, Kumar S, Ojo T, Knepler J. Ultrasound for critical care physicians: characteristic findings in a complicated effusion. Southwest J Pulm Crit Care. 2018;17(6):150-2. doi: https://doi.org/10.13175/swjpcc122-18 PDF
 Post a Comment
Post a Comment
Reader Comments